Universal Health Care refers to a national system that would provide medical benefits and services to all citizens, regardless of ability to pay. Read the overview below to gain an understanding of the issue and explore the previews of opinion articles that highlight many perspectives on universal health care.
"Universal Health Care." Gale Opposing Viewpoints Online Collection, Gale, 2019.
Universal health care refers to a national health care system in which every person has access to medical services. Though universal health care can refer to a system administered entirely by the government, most countries achieve universal health care through a combination of state and private participants that comprises hospitals and clinics, health care practitioners, insurance providers, and employer-supported programs. Each country institutes universal health care according to its own needs and capabilities. Systems funded entirely by the government are considered single-payer health insurance. As of 2020, single-payer health care systems could be found in seventeen countries including Canada, Norway, and Japan. In some single-payer systems, such as the National Health Services in the United Kingdom, the government provides health care services. Under most single-payer systems, however, the government administers insurance coverage, while nongovernmental organizations, including private companies, provide treatment and care. Other universal health care systems require that all eligible citizens purchase private insurance as a means of ensuring total coverage. Critics of such programs contend that insurance mandates force people to purchase insurance, undermining their personal freedoms.
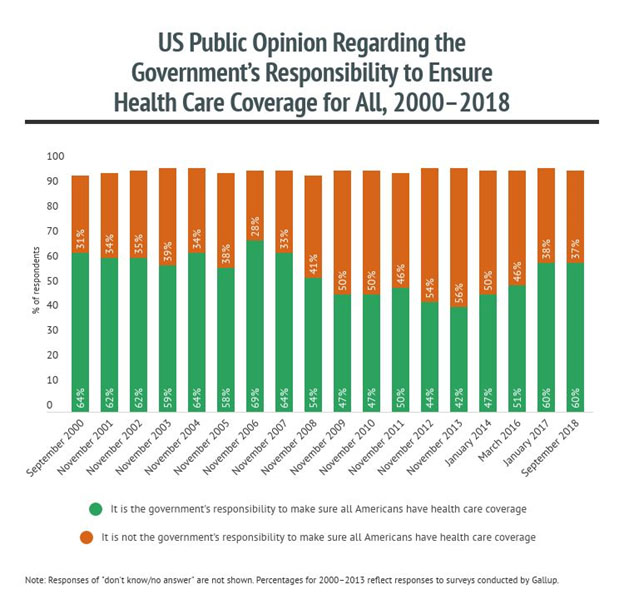
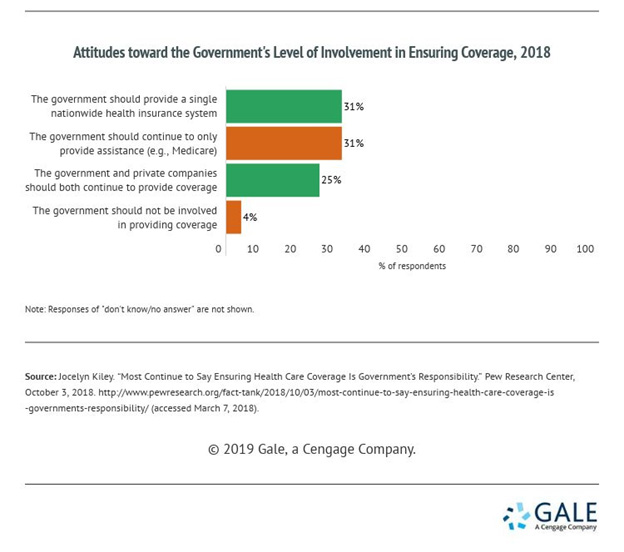
The United States has struggled both with ensuring health coverage for the entire population and with reducing overall health care costs. Policy makers have sought to address health care at the local, state, and federal levels with varying degrees of success. Universal health care became a subject of debate in the 2020 presidential election, with the Democratic candidate Joe Biden, who won the election, including universal health care as part of his platform. Alternatively, President Donald Trump and other members of the Republican Party have characterized such proposals as economically implausible and threatening to individual choice. A 2020 report by the Pew Research Center found that 63 percent of Americans believe the federal government should be responsible for ensuring all Americans have health care coverage. Universal health care remains a partisan issue, with 54 percent of Democrats supporting a single-payer health care system and 66 percent of Republicans believing that the government does not have a responsibility to ensure people have health care coverage.
In 2020 the novel coronavirus disease (COVID-19), a highly contagious respiratory infection, spread to more than 190 nations and overwhelmed health care systems around the world. By the end of 2020 more than 20 million Americans were confirmed to have been infected with the virus that causes COVID-19 and at least 350,000 Americans had died. The pandemic illuminated inadequacies in the country's health care system, such as the disparities in social protections and structural inequalities for people in low-income and marginalized communities.
Cons
Bill Clinton campaigned for president on a platform that included health care reform in 1992. Similar proposals had been made earlier, as universal health care was also part of the platform of Jesse Jackson's failed 1988 presidential bid. Shortly after arriving in office, Clinton established the Task Force on National Health Care Reform, with his wife, Hillary, serving as its chair. The First Lady's involvement led some to refer to the Health Security Act of 1993, which the task force helped develop, as "Hillarycare." The proposal would have required all individuals to acquire health insurance and all employers of more than five thousand people to provide health coverage to their employees. The bill met with opposition from policy makers, insurance companies, and physician groups, and did not pass. The failure of Clinton's efforts led many officials to view health care reform as an issue too complicated and too contentious to risk losing any political influence over. In contrast to the Health Security Act, Representative Jim McDermott (D-WA) introduced the similarly named American Health Security Act in 1993, which would have created a single-payer system. McDermott reintroduced the bill at each session of Congress until choosing not to seek reelection in 2016.
In the early twenty-first century, state and federal officials showed renewed interest in expanding health care coverage. In 2003 Representative John Conyers Jr. (D-MI) first introduced the United States National Health Insurance Act, which called for a single-payer health care system, but the bill received neither a debate nor a vote on the House floor. Like McDermott, Conyers continued to introduce the bill at every subsequent session of Congress until he resigned from office in 2017. While the federal government took little action toward achieving universal health care, state legislators experienced success in expanding health coverage in Massachusetts in 2006. The Massachusetts system mandated that every citizen obtain health insurance or pay fines. The system is sometimes called "Romneycare" in reference to Mitt Romney, who served as governor during its implementation. The reform led Massachusetts to achieve 98 percent health coverage within four years, higher than any other state. Experts have attributed the success of the Massachusetts system to government subsidies, which enabled more people to purchase insurance, and to the program's insurance mandate, which appealed to insurance companies because they acquired more customers.
In 2008 Barack Obama campaigned on health care reform in his bid for president, drawing heavily on the Massachusetts model. Upon winning office, Obama made expanding health coverage a central focus of his presidency. The efforts of his administration led to the passage of the Patient Protection and Affordable Care Act (ACA), often referred to as "Obamacare," in 2010. According to the Centers for Disease Control and Prevention (CDC), the percentage of Americans who did not have health insurance for more than one year dropped from 16.8 percent in 2010 before the law went into effect to 7.6 percent in the final year of Obama's presidency. Despite the law's effectiveness in reducing the number of people without health coverage, some critics of the system note that some individual premiums increased and that, due to the subsidies to cover insurance premiums that were allocated based on income, the system's benefits were disproportionately experienced by low-income and older enrollees not yet eligible for Medicare and enrollees with pre-existing conditions. Alternatively, some critics considered the overhaul of the health care system insufficient, contending that a single-payer system would better serve the population.
Vermont senator Bernie Sanders, whose 2016 presidential bid emphasized health care reform, introduced the Medicare for All Act of 2017, a proposal to expand government health insurance coverage to all citizens and residents. In July 2018 more than seventy Democratic members of the House of Representatives formed the Medicare for All Caucus to sponsor briefings on health care reform. One of the caucus's co-founders, Pramila Jayapal (D-WA), introduced a resolution outlining a single-payer national health insurance program in February 2019. As support for a single-payer system has grown among progressive factions within the Democratic Party, some critics, including fellow Democrats, have argued that a health care system without a role for private insurance could lead to a decrease in quality of service.
In November 2020 Biden won the presidential election. He emphasized that health care issues would have a prominent position in his administration's agenda. During his campaign, he pledged to expand ACA by expanding federal subsidies to help cover insurance premiums for a greater portion of the population. His campaign's health care plan also included a Medicare-like health insurance program, or a "public option" that would be administered by the federal government.
A frequently cited study conducted by researchers at Harvard Medical School and Cambridge Health Alliance in 2009 determined that almost forty-five thousand Americans die each year due to problems related to their lack of health insurance. Proponents of universal health care contend that these deaths could be avoided, as everyone would be covered. By ensuring that citizens and residents have access to affordable medical services, universal health care can improve overall public health by treating the sick, promoting preventative care, and providing basic care to all patients. Critics warn, however, that universal health care could lead to decreased quality of care and long wait times. A commonly cited fear associated with single-payer systems relates to the rationing of medical services, which refers to the limiting of health care services based on the availability of resources.
In response to concerns over rationing, some medical experts and economists assert that rationing exists in all health care systems because resources are always limited. In the United States, however, how these resources are rationed is determined by patients' abilities to pay rather than their medical needs. Discrepancies in medical treatment throughout the United States also suggest that access to medical services can be dependent on where patients live and where they are employed as well as demographic factors such as race, gender, and ethnicity. Some health care experts have argued that the Medicare system in the United States can be characterized as an explicit form of health care rationing because the program only provides coverage to people ages sixty-five or older, people with certain disabilities, and people with end-stage renal disease. Proponents of expanding Medicare coverage contend that doing so will make access to health care more equitable.
Many critics of universal health care cite the potential costs of implementation as the primary reason for their opposition. Some critics of universal health care have voiced concern that a single-payer system would lead to people seeking unnecessary treatments and that the overuse of services would drive overall costs up. Proponents, however, counter this argument by suggesting that the increased use of preventative services would reduce the need for expensive treatments because health issues could be identified earlier.
In 2018 researchers at the Mercatus Center at George Mason University conducted a study to determine the cost of implementing the Medicare for All Act of 2017. Opponents of single-payer health care initially celebrated the results, which showed Sanders's plan would cost $32.6 trillion over the first ten years. However, Sanders responded by noting that the report's total indicated an overall savings of $2 trillion compared to spending projections without implementing reforms. Proponents of the plan expect some of these savings would be derived from a reduction in administrative costs by eliminating private insurance organizations from the process and decreasing the amount of unneeded paperwork. The Mercatus Center report warns, however, that government programs tend to accrue significant administrative costs and that government-run health care may likely incur similar costs, making projected savings uncertain.
In 2020 the COVID-19 crisis exacerbated vulnerabilities in the US health care system. The country lagged behind in pandemic readiness, especially compared to nations with universal health care systems. The United Nations (UN) warned that the pandemic revealed shortcomings in health care systems worldwide. In October 2020 the UN secretary-general, António Guterres, called for global investment in universal health care, identifying the gap in health coverage as one of the causes for the devastating effects of the COVID-19 pandemic. An October 2020 UN policy brief highlighted the long-term economic effects of underinvestment in health care. The statement estimated the monthly cost of the pandemic to the global economy at $375 billion, noting that millions of people had been infected, and hundreds of thousands had lost their lives. The UN warned that disparities in treatment and fragmented health care systems cause individual suffering and larger social and economic challenges.
"This is a struggle against the 'economic royalists', as Franklin D Roosevelt once termed them, of our day—and for the interests of ordinary working people."
Adam Gaffney is an instructor at Harvard Medical School, a pulmonary and critical care doctor at Cambridge Health Alliance, and president of Physicians for a National Health Program. He blogs at the Progressive Physician.
In the following viewpoint, Gaffney disputes US conservatives' common argument against universal health care that the costs to implement and sustain such a system make it unaffordable. Citing research from both ends of the political spectrum, the author indicates that single-payer policies like Medicare for All would save the country trillions of dollars over a decade. Further, Gaffney suggests, the unaffordability argument against single-payer health care persists despite evidence of its inaccuracy because corporations and the wealthy have disproportionate control and influence over US politics. The author concludes that Democratic and progressive proponents should focus more of their messaging on the positive impact that universal health care has on broader socioeconomic inequities.
"'Affordable health care for all' from government is an economic oxymoron."
Eric Rozenman is a communications consultant for the Jewish Policy Center in Washington, DC.
In the following viewpoint, Rozenman argues that single-payer universal health care is unrealistic because it would cost too much for the country to implement and maintain. Because of high costs, the author suggests, the resulting system would require the government to delay people's access to care and could lead to rationing. The author claims that Democratic politicians' support for universal health care is disingenuous, implying that it represents a tactic to obtain power under the guise of acting in the interest of citizens' welfare. Rozenman concludes that universal health care would effectively turn all citizens into wards of the state, which conflicts with American individualism and could restrict economic prosperity.
"Access to government health insurance does not automatically translate into access to medical care."
Robert Moffit is a senior fellow in domestic policy studies at the Heritage Foundation, a conservative public policy organization based in Washington, DC.
In the following viewpoint, he opposes the single-payer health care proposals advocated and introduced by Democratic lawmakers that are commonly referred to as "Medicare for All." Citing problems in the British and Canadian single-payer national health care systems, Moffit argues that access to care in the United States would worsen under a Medicare for All plan. The author acknowledges that there are serious problems in the US health care market but maintains that a single-payer Medicare for All reform would fail to solve those problems and could negatively impact the aspects of US health care that citizens indicate are working well for them.
"Other high-income countries spend less on health care than the United States because they have lower prices, not because they receive less care."
Jamie Daw is assistant professor of health policy and management at the Mailman School of Public Health at Columbia University in New York.
In the following viewpoint, Daw argues that US politicians should look to Germany's model of social health insurance for inspiration rather than Canada's single-payer model. She notes that the German system for universal health care has been developed and tested over time, with many other European and Asian countries adopting similar models. Because the German system is multipayer, Daw contends, it provides a better example for US policymakers to use when advocating an American universal health care system. The author concludes that a hybrid system of publicly and privately funded plans can meet the goals of universal affordable coverage without eradicting the private health care industry, which many Americans cite as a reason for their opposition to single-payer proposals.